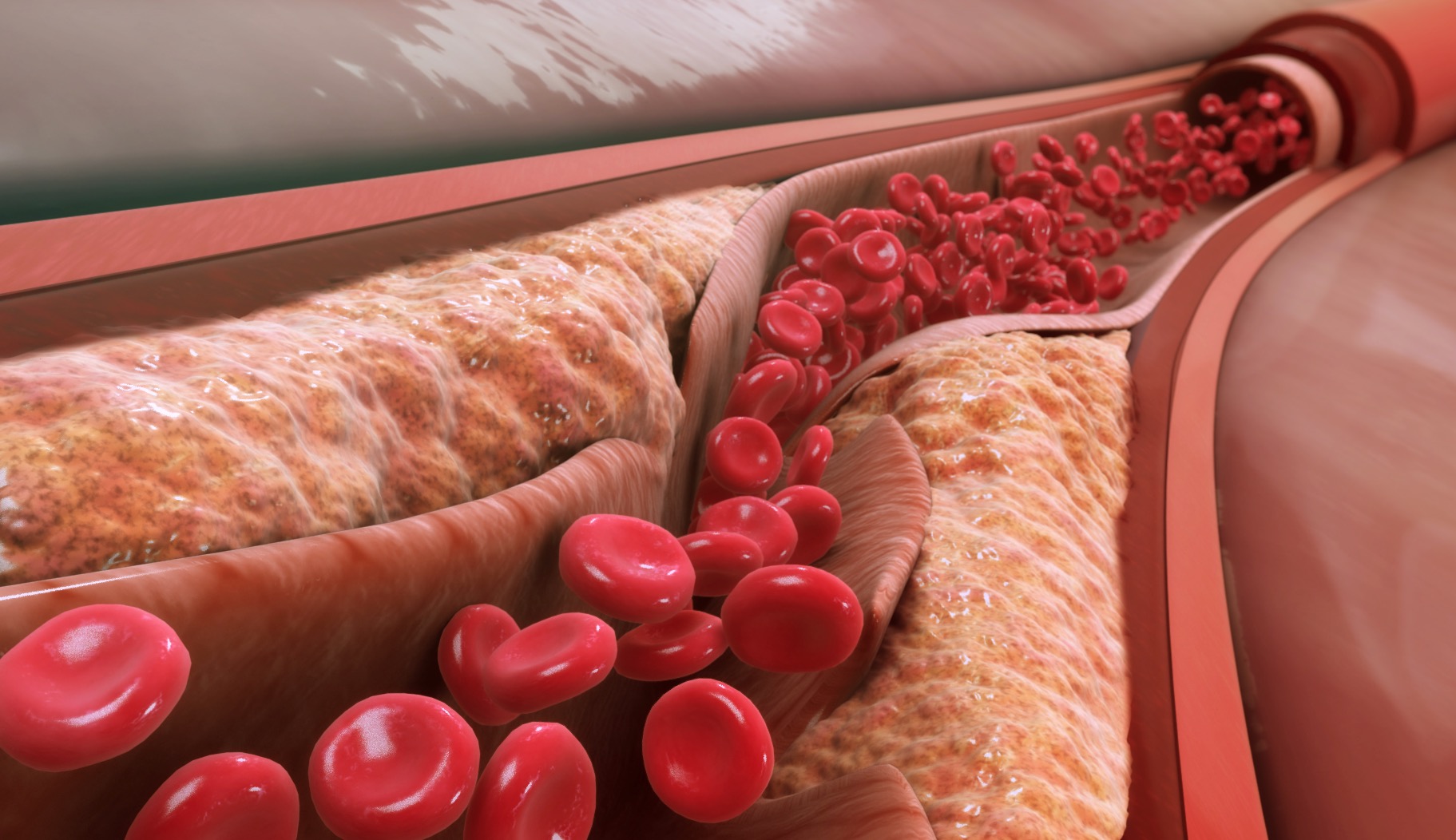
Tibial chronic total occlusions (CTOs) are among the most technically demanding challenges in peripheral intervention. These lesions are often long, calcified, and angulated—and yet they lie at the very heart of limb salvage efforts in patients with chronic limb-threatening ischemia (CLTI).
While recanalizing tibial CTOs may not offer the glamour of coronary work or aortic interventions, it is often what determines whether a patient walks or undergoes amputation.
In this post, we break down the strategies, tools, and practical pearls that help clinicians successfully cross and treat tibial CTOs.
Why Tibial CTOs Are So Challenging
Tibial CTOs often arise in patients with:
- End-stage diabetes or renal disease
- Diffuse atherosclerosis with severe calcification
- Previous failed bypass or endovascular attempts
They’re usually:
- Long (>10 cm)
- Heavily calcified, sometimes circumferential
- Located in small (<3 mm) vessels
- Associated with poor inflow or distal runoff
Crossing is only part of the battle—creating a durable result that restores perfusion to the wound bed is the ultimate goal.
Step 1: Understanding the Anatomy
Pre-procedure planning is essential.
Imaging Essentials:
- High-resolution duplex ultrasound or CT angiography
- Angiographic roadmap with both anterior and posterior tibial visualization
- Assessment of pedal arch for reentry options
Clinical Tip: Always identify at least one target vessel with good distal outflow to the ulceration or amputation site.
Step 2: Crossing Techniques — Building Your Strategy
- Intraluminal Approach (First-Line)
- Best for short to moderate CTOs without heavy calcification
- Use hydrophilic guidewires (e.g., Glidewire, Command) with supportive catheters
Progress gently; avoid forceful push that risks subintimal entry or perforation.
- Subintimal Tracking
- Unintentional entry is common—learn to work with it
- Use looped tip of a wire to create a plane, then re-enter distally
- Use support catheters (e.g., Quick-Cross, CXI) to follow wire
Subintimal techniques require finesse, especially in small-caliber tibials.
- Retrograde Pedal Approach
When antegrade fails, retrograde works:
- Access dorsalis pedis, lateral plantar, or posterior tibial arteries
- Use 21G needle and 0.018″ or 0.014″ wire
- Advance wire retrograde and meet antegrade system (“flossing”)
Retrograde access requires precision and ultrasound guidance—but in expert hands, it dramatically increases CTO crossing success.
Step 3: Tools of the Trade
|
Tool
|
Use Case
|
|
Hydrophilic 0.014–0.018″ wires
|
First-line crossing (Command, Pilot, Fielder)
|
|
Support catheters
|
CXI, Quick-Cross, Turnpike – essential for torque
|
|
Reentry devices (limited tibial use)
|
Off-label or specialized settings
|
|
Micropuncture kits
|
Pedal access and low-profile entry points
|
|
Atherectomy
|
For severe calcification prior to balloon angioplasty
|
Always start with low-profile, highly steerable systems, and escalate only as needed.
Adjunctive Therapies After Crossing
Crossing is step one—definitive therapy requires durability.
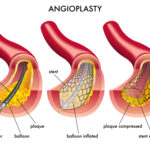
- Low-profile balloon angioplasty is standard
- Consider drug-coated technologies when available
- Avoid stenting unless absolutely necessary—stent fractures and occlusion risk are high in tibials
- Evaluate pedal loop for complete revascularization
Goal: Achieve direct flow to the angiosome of tissue loss. Revascularizing indirect vessels offers less wound-healing potential.
Success Metrics and Outcomes
- Technical success rates: 70–90% with combined antegrade and retrograde approaches
- Limb salvage improves significantly with tibial CTO revascularization—especially when angiosome-directed
- Patency rates are modest, but even short-lived revascularization can heal wounds and delay amputation
Final Thought: Persistence with Precision
Tibial CTOs may test the patience and creativity of any operator. But for patients facing limb loss, crossing a 20 cm calcified artery may mean restoring life and mobility.
Success comes not from brute force, but from planning, finesse, and the willingness to try every pathway—antegrade, retrograde, subintimal, and beyond.
At TriVasc Academy, we advocate for a stepwise, anatomy-driven approach, supported by real-world case experience and advanced techniques—so more patients keep their limbs, and their independence.
Coming Soon at TriVasc Academy:
Pedal access masterclass videos
Tibial CTO algorithm cards
Angiosome-targeted revascularization planner