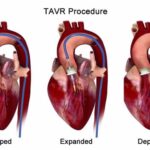
As transcatheter aortic valve implantation (TAVI) becomes the gold standard for treating aortic stenosis across a growing range of patient risk categories, new challenges are emerging—chief among them, conduction disturbances.
Despite procedural success, atrioventricular (AV) block, new-onset left bundle branch block (LBBB), and high-degree heart block remain common complications after TAVI. These electrical disruptions can impact long-term patient outcomes, mandate permanent pacemaker implantation (PPI), and even affect mortality.
In this blog, we unpack the why, who, and when of post-TAVI conduction issues—and how a thoughtful approach to monitoring and pacing can improve care.
Why Do Conduction Disturbances Occur After TAVI?
The aortic valve annulus lies in close proximity to the His-Purkinje conduction system, particularly along the membranous septum. Mechanical stress, radial force, and local trauma during valve implantation can easily disrupt electrical conduction, especially with:
Incidence and Clinical Relevance
While many disturbances resolve spontaneously, some persist—and inappropriately timed pacemaker decisions may lead to unnecessary device implantation or sudden deterioration.
Key Risk Factors for Post-TAVI Conduction Disturbance
|
Patient Factors |
Anatomical Factors |
Procedural Factors |
|
Pre-existing RBBB or bifascicular block |
Short membranous septum |
Deep prosthesis implantation |
|
Baseline PR or QRS prolongation |
Heavy LVOT or annular calcification |
Valve oversizing |
|
Older age and frailty |
Small aortic annulus |
Use of self-expanding valve systems |
Clinical Tip: Patients with RBBB and baseline prolonged PR interval are at the highest risk for complete heart block post-TAVI.
Post-TAVI Monitoring Strategy
A structured monitoring plan is essential to guide appropriate pacing decisions.
In-Hospital Monitoring (Day 0–3)
If LBBB develops, monitor for QRS widening and symptoms of AV block.
🔬 High-Risk Indicators During Monitoring:
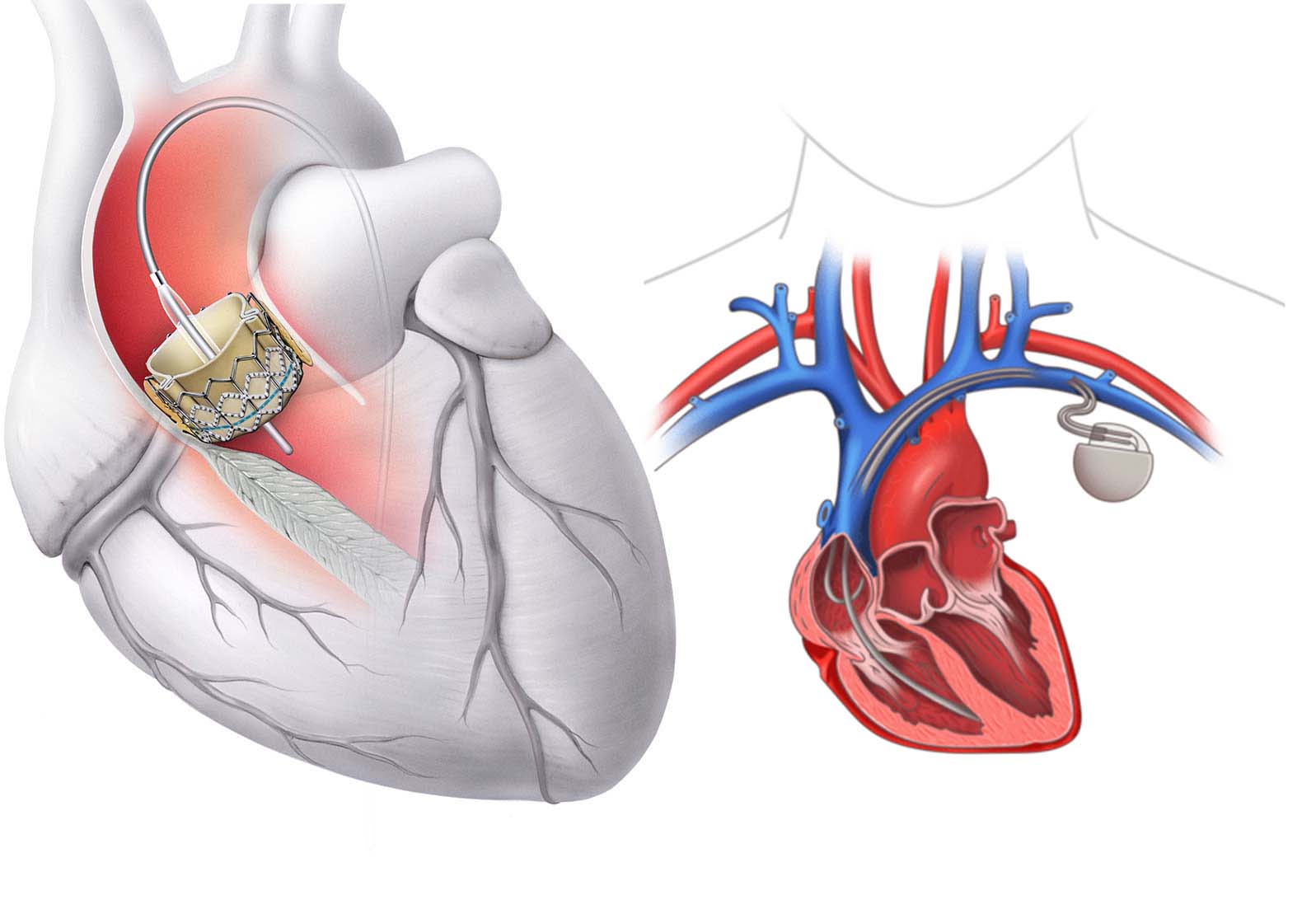
When Should You Implant a Permanent Pacemaker?
Clear Indications (Implant Immediately):
Watchful Waiting (With Close Monitoring):
Suggested Observation Period: 48–72 hours post-TAVI for borderline cases; consider ambulatory Holter or ILR if early discharge is planned.
Valve Type and Pacing Risk
|
Valve Type |
Pacing Risk Profile |
|
Self-expanding (e.g., CoreValve) |
Higher risk (~15–25% PPI rate) |
|
Balloon-expandable (e.g., Sapien) |
Lower risk (~5–10% PPI rate) |
|
Mechanically-expandable (e.g., Lotus) |
High risk but withdrawn from market |
Implantation depth matters more than valve type alone. Deep placement (≥6 mm below annulus) significantly increases conduction risk.
Long-Term Implications of Post-TAVI Pacing
While pacemakers prevent bradyarrhythmic complications, they are not benign. Chronic RV pacing has been associated with:
This underscores the need to avoid unnecessary implantation and consider alternatives such as His-bundle or biventricular pacing in select patients.
Final Thought: Balance Speed with Strategy
TAVI teams must walk a fine line between reacting to early conduction changes and premature pacemaker implantation.
The key is structured monitoring, individualized risk assessment, and clear pacing algorithms.
At TriVasc Academy, we emphasize a team-based, evidence-informed approach to conduction management—because saving a heart valve means little if we destabilize the heart’s rhythm in the process.
Coming Soon at TriVasc Academy:
Post-TAVI conduction monitoring checklists
Pacemaker implantation decision trees
Annotated ECGs and real-world case series